
Orthotopic Liver Transplant:Post Operative Imaging with Ultrasound
Mindy M. Horrow, MD, FACR, FSRU, FAIUM
Director of Body Imaging, Einstein Medical Center
Philadelphia, PA
Professor of Radiology
Thomas Jefferson Medical College
Surgical Technique
•End to end arterial anastomosis using Carel patch ofdonor aorta or hepatic artery and recipient hepatic artery
–Variant anatomy
–If insufficient inflow from native hepatic artery, may use donor iliacartery interposition graft anastomosis to infra-renal aorta
•End to end portal vein anastomosis between donor andrecipient portal veins
–With recipient portal vein thrombosis, portal inflow can beestablished using an iliac vein interposition graft from the superiormesenteric, splenic or renal veins
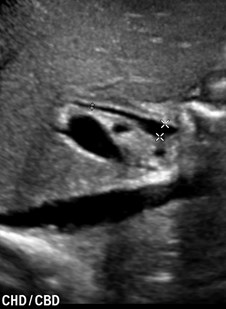
•End to end biliary anastomosis, occasional T-tube,Cholecystectomy
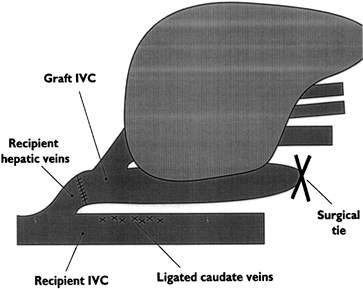
•IVC anastomosis: “piggy-back” currently favored, creatinganastomosis between supra hepatic donor IVC andrecipient hepatic venous confluence
Post Operative Ultrasound Evaluation
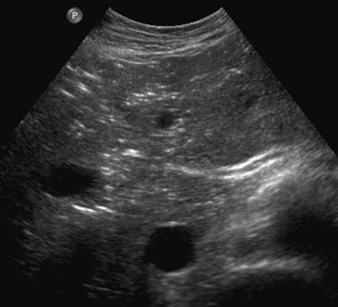
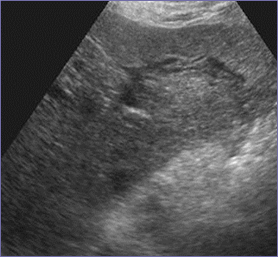
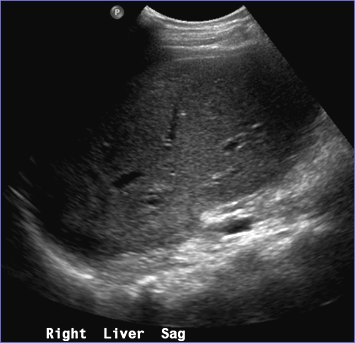
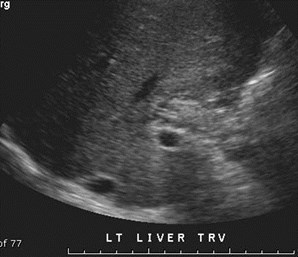
•Gray Scale imaging of liver, perihepatic space
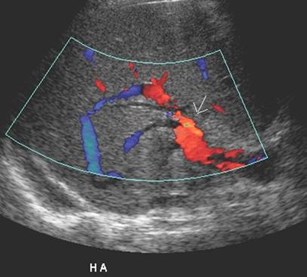
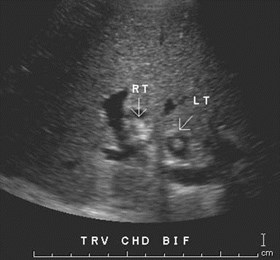
•Hepatic Artery
–Porta hepatis, right and left intra-hepatic arteries, anastomosis ifpossible
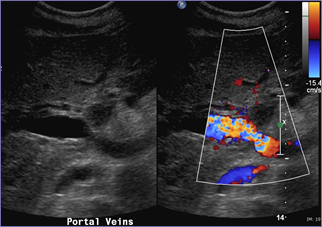
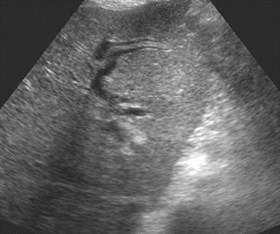
•Portal Vein
–Main portal vein, left and right intra-hepatic branches
•IVC and Hepatic Veins (right, middle and left)
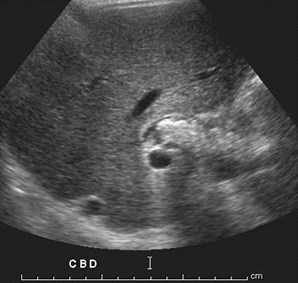
•Bile Duct
Bhargava, etal AJR 2011;196:WS15
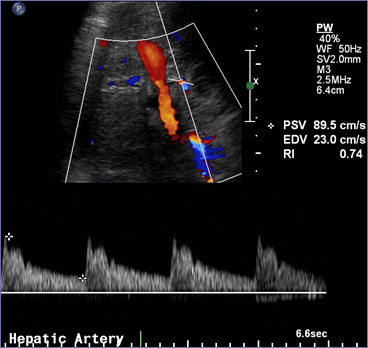
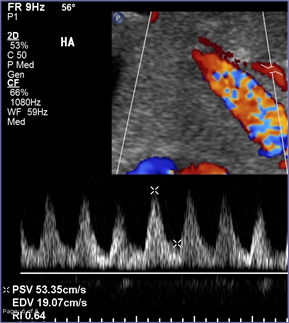
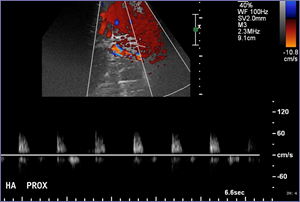
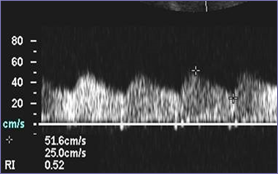
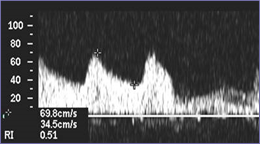
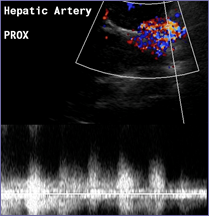
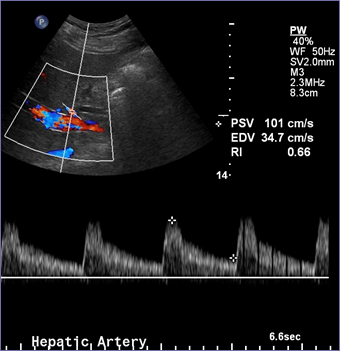
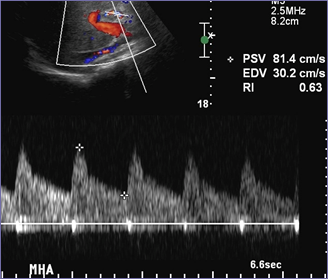
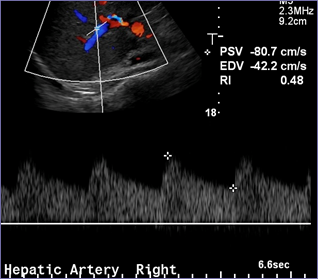
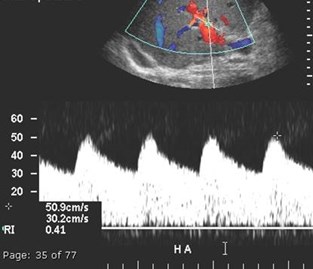
Hepatic Artery
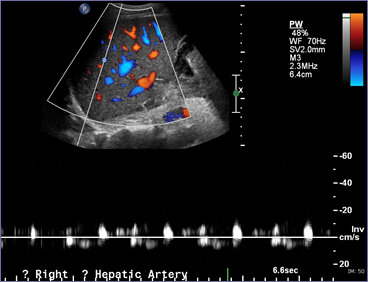
1.Prompt systolic upstroke withacceleration time (time fromend diastole to first systolicpeak) < 100 msec
2.Continuous flow throughoutdiastole
3.Resistive index between 0.55and 0.8
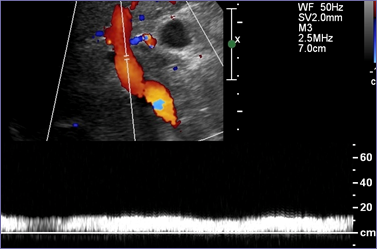
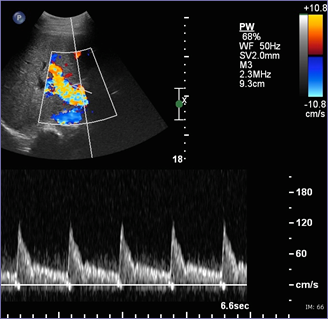
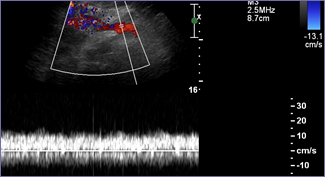
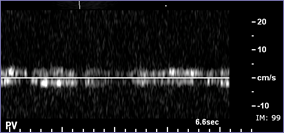
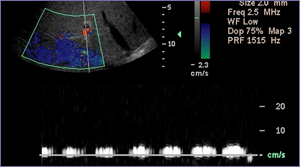
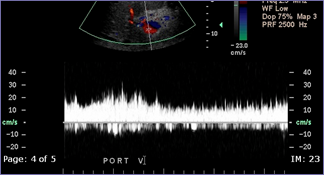
Portal Vein
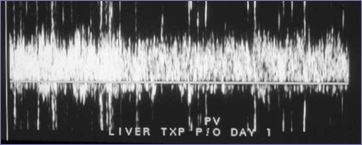
1.Antegrade flow, sometimes turbulent inimmediate post operative imaging
2.Slight fluctuation due to respiratory variability
3.Maximum velocity range 13 – 30 cm/sec
4.Minimum velocity range 6 – 20 cm/sec
5.RI 0.39 0.1
Barakat BrJRad 2002;75:417
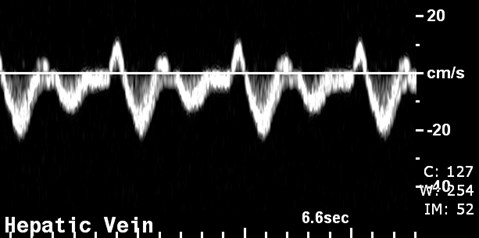
Hepatic Vein
1.Atrial and ventricular systole
2.Atrial and ventricular diastole
3.Deep inspiration increases abdominal pressurereducing mesenteric blood flowing toward heart.This causes a dampening of normal phasicity.
Abu-Yousef JUM 1992;6:263
Initial “near normal” findings
•Hepatic artery high resistance flow
•Portal vein
–Recipient-donor size mismatch
–Helical flow
–Portal venous gas
•Loss of hepatic venous pulsatility
•Other
Brody, Horrow, etal. US Q. 2008;24:257
Day 1 Day 3
Initial high resistance waveform Spontaneous normalization

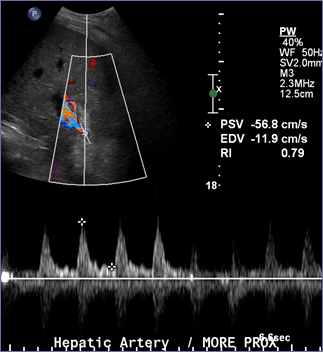
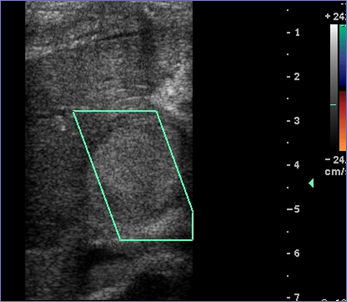
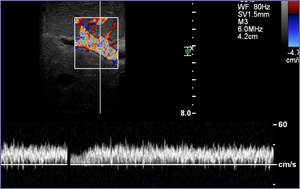
Early High Resistance Arterial Flow
•High resistance flow, even with RI=0, notuncommon in first few days after surgery
•Not associated with poor clinical course ordecreased survival
•Longer cold ischemia times and older donorsindependently associated with elevated RI
•Possible association with chronic cholestaticdisease as indication for transplantation
•If concerned can administer a vasodilator
Garcia, etal. AJR 2003;181:831
Chen, etal. JUM 2006;25:631
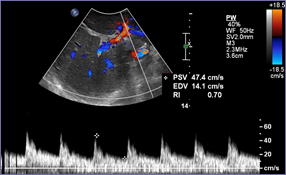
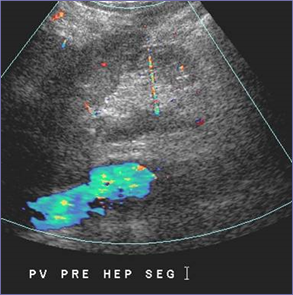
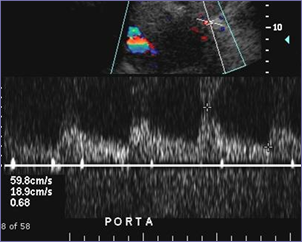
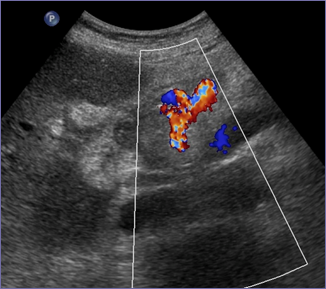
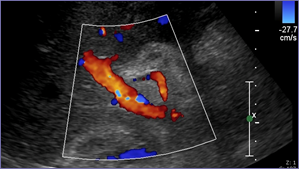
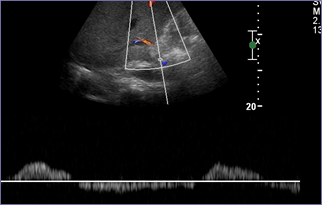
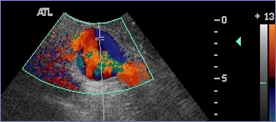
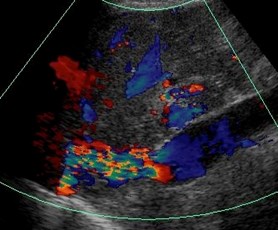
Immediate Portal Vein “Stenosis” withspontaneous resolution

Immediate post op One year later
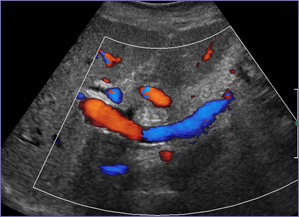
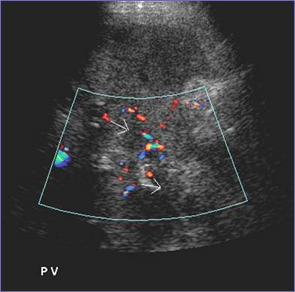
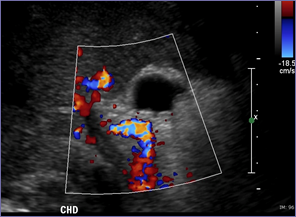
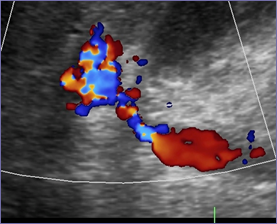
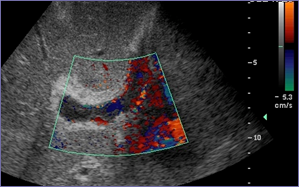
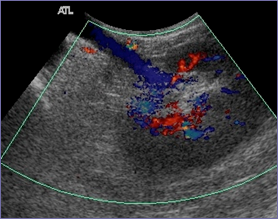
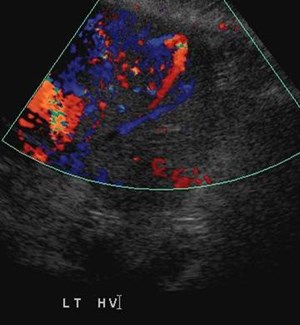
Helical Portal Vein Flow
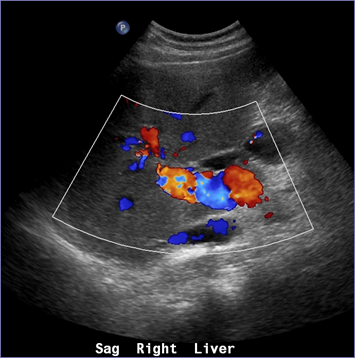
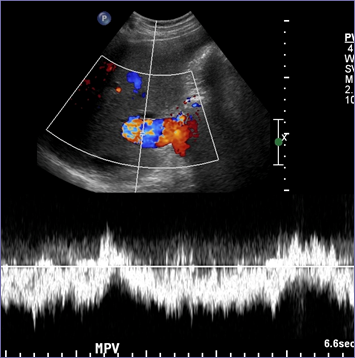
Helical Portal Vein Flow
•Spiral flow in an overall hepatopetaldirection
•May be seen in up to 43% after liver tx
•More common with size discrepancybetween donor and recipient portal veins
•Alternating parallel red and blue bands
•Pulsed Doppler tracing varies with locationof cursor
Brody, Horrow, etal. US Q. 2008;24:257
Friedewald, etal, US Q. 2003;19:71
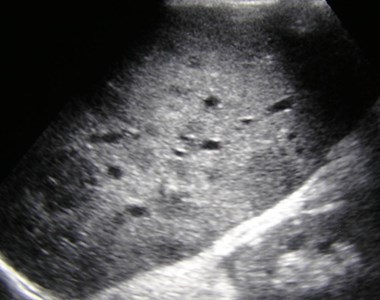
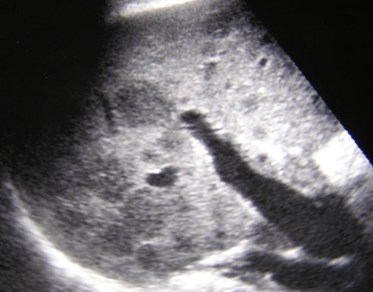
Portal Venous Gas

Chezmar, etal. AJR 1989;153:1203
Uncommon but likely
Insignificant finding.
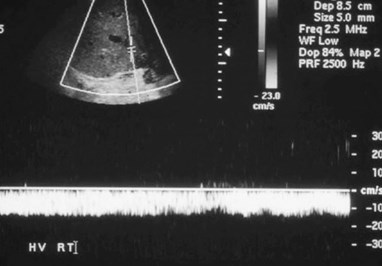
Loss of hepatic venous phasicity
1.Sensitive, but non-specific indicator of rejection.
2. Triphasic flow helps eliminate possibility of rejectionwith high negative predictive value (92%).
Jequier, etal. Radiology 2003;226:105
Small resolving perihepatichematoma
Day 1
Day 12
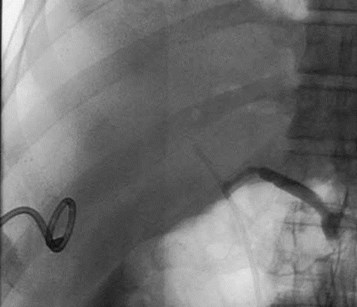
Free air- immediately aftersurgery

Clip fromcholecystectomy


Hepatic Artery Complications
•Thrombosis
–Early- immediate post-operative
–Late
•Biliary complications
•Collateralization
•Stenosis
•Other
–Pseudoaneurysm
–Arcuate ligament syndrome
–Arterio-venous fistula
–Splenic artery steal
–Initial low resistance
Hepatic Artery Thrombosis
•Incidence: 3-5% in adults, 9-42% inchildren
•Clinical: non-specific
•Risk Factors:
–prolonged cold ischemia, donor-recipient HAmismatch, small caliber, interposition grafts,CMV infection, acute rejection
•Associated complications:
–Bile leak, non-anastomotic biliary strictures,liver infarction or abscess, recurrentbacteremiaor cholangitis
Langnas, etal Am J Surg 1991;161:76
Nolten, etal. Radiology 1996;198:553-539
Wozney, etal AJR 1986;147:657
Hepatic Artery Thrombosis
•Screen with duplex Doppler
–Sensitivity and specificity ~ 87- 92%
•Early- near 100% sensitivity
•Late 73% sensitivity
•CTA, MRA and conventional catheterAngiography for confirmation and confusingcases
•Microbubble contrast to improve sensitivity
Horn, etal. Radiology 2006;241:267
Horrow, etal AJR 2007;189:346
Kim, etal Abdom Imaging 2007;32:635
Nolten, etal. Radiology 1996;198:553-539
Flint, etal AJR 1988;151:481
Early versus Late HAT
•Early thrombosis < 1 week is usually considereda surgical complication, requiring surgicalrevascularization
–Clinical: acute graft failure, sepsis, liver abscess, biliarycomplications
–Lack of flow is best indicator in peri-operative period.
–US more sensitive
•Late thrombosis 1 week due to a variety offactors
–Clinical: cholangitis with or without strictures or abscesses,bile leaks, or may remain clinically silent with abnormal LFTs
–US less sensitive
Hedegard, etal US Q 2011;27:49
Horrow, etal AJR 2007;189:346
Silva, etal. Liver Trans. 2006;12: 146-151
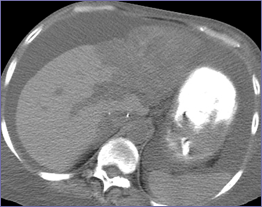
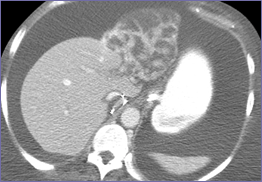
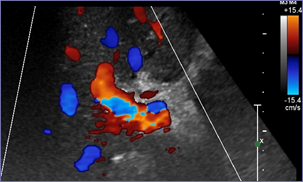
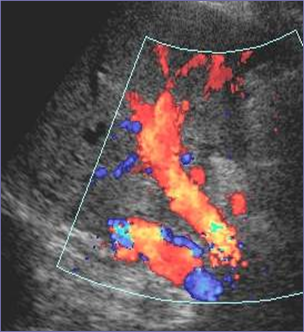
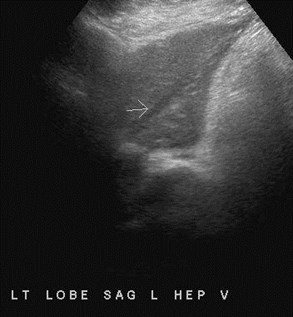
Routine post operative US, 8 hours post tx

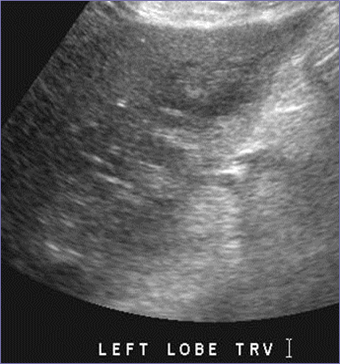
Absent hepatic arterial flow, abnormal left lobe
Hepatic artery thrombosis, patient returns foremergency surgical thrombectomy

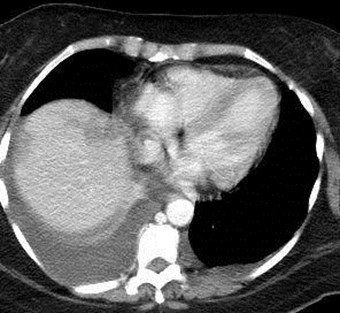
Immediate post thrombectomyUS and subsequent CTs
Day 11
Day 16
2 mos.
Infarction left lobe of liver
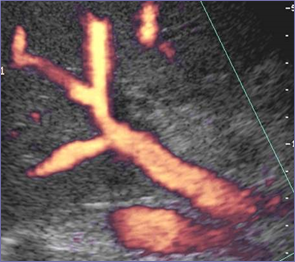
Impending HAT first post tx US
Intraoperative post unkinking of HA
Few hours post thrombectomy
Very difficult to visualize HA
Still high resistance but muchbetter velocities
Dissection RHA related to procedure

2 weeks later- asymmetric L and R hepatic arteries
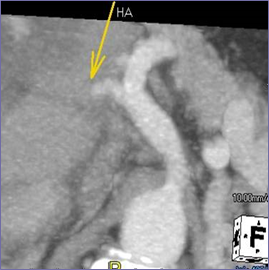
HA
POST OP DAY 1
POST OP DAY 15
Hepatic ArteryThrombosis
POST OP DAY 15 POST OP DAY 25
Development of Bilomas


Follow up with drainage of infected, sludgefilled bile ducts
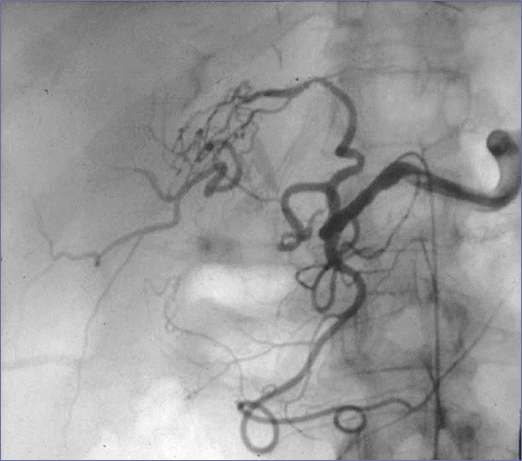
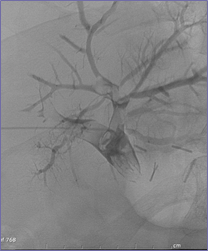
Several months laterafter biloma and biliarydrainage, diffuse portalvenous thrombosis.
Interval Development of arterial collaterals





Exuberant arterialcollaterals predominantlyfrom SMA, main PVthrombosis

11/11 12/06
Patient with rising LFTs 2 years after transplant

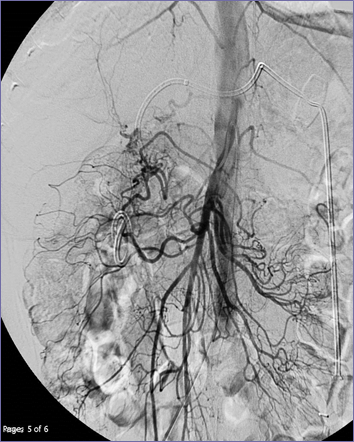
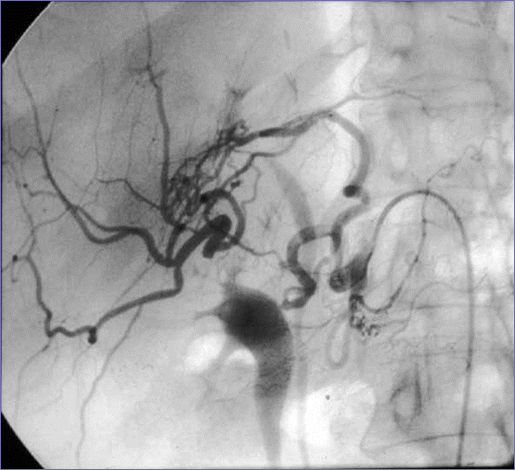
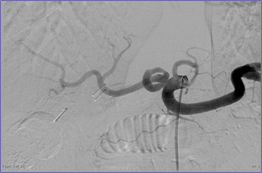
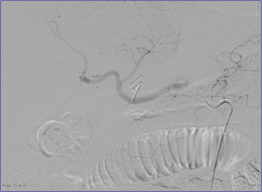
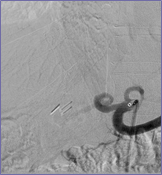
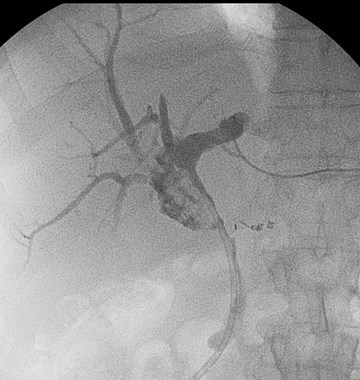
Late HAT with arterial collaterals

Dilated, sludge filled ducts
Late HAT and arterial collaterals
•Sonography becomes less sensitive for HAT as timefrom transplant increases because of collateralization.
•Collateral arterial waveforms may be parvus tardus andsimulate hepatic artery thrombosis
•Collateral arterial waveforms may be indistinguishablefrom normal, so called “Collateral transformation of thehepatic artery”
•Suspicion for this complication should increase if : intra-hepatic biliary dilatation, sludge, bilomas, pattern similarto sclerosing cholangitis
•Probably a more common occurrence than recognizedwith some asymptomatic patients.
Dydynski, etal. AJR 2008;191:546
Horrow, etal. AJR 2007;189:346-351


Abnormal LFTs
Left HA
Right HA
Thrombosed right hepatic artery branch with left branchsupplying right lobe. Parvus tardus waveform from right sidebecause of collateral filling.

LHA
Coil embolization of gastro-duodenal arteryimproves flow to left hepatic artery branch andthrough collaterals to right lobe.

Initial low hepatic artery resistiveindex
•May be a predictor for subsequent vascularcomplications, including hepatic artery, portalvein, hepatic vein and IVC
•Persistently low RI more significant than atransient finding.
•Recommendation to carefully monitorperioperative patients with resistive index < 0.6
Hedegard etal. US Quarterly 2011;27:49
Uzochukwu etal. AJR 2005;185:1558
Hepatic Artery Stenosis
•Second most common arterial complication in 5 – 11%
•Typically occurs at anastomosis
•Can cause ischemia, biliary complications and progressto thrombosis and graft loss
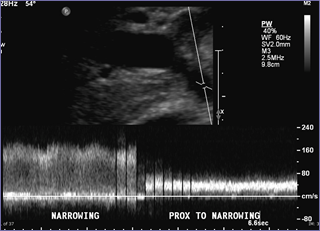
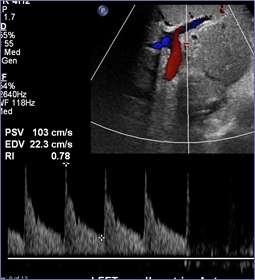
•If stenotic site is visible, velocities elevate to > 200cm/sec with distal parvus tardus waveform
•Pitfalls include: tortuosity, HAT with collaterals, celiacstenosis and intra-hepatic arteriovenous fistula
•Low grade stenosis may not cause significant Dopplerabnormality, so if high clinical suspicion (biopsy withischemia) proceed to CTA, MRA or catheter angiography
Dodd etal. Radiology 1994;192:657
Vaidya, etal. US Quarterly 2007;23:239
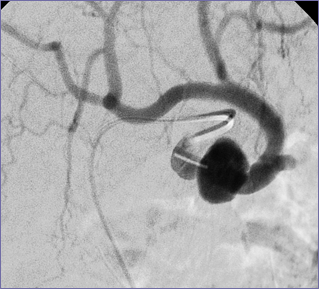
Hepatic artery stenosis
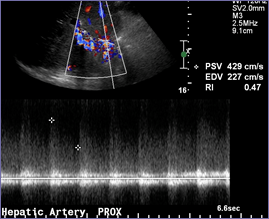
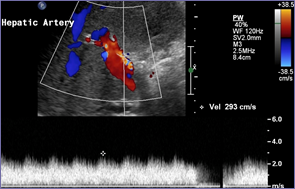
Proximal At Stenosis
Post stenotic
Parvus tardus waveform
Color Bruit
Pre and post angioplasty
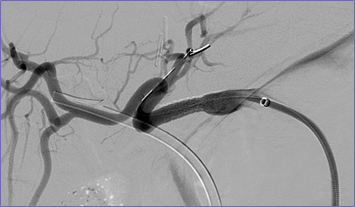
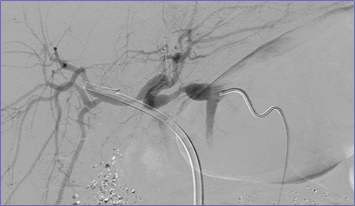
Some improvement in waveform
Immediately post angioplasty

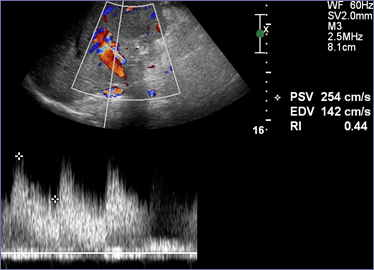
Patient with rising LFTs
Waveforms not very abnormal, but distally withslight delay in upstroke and decreasing resistiveindex
Regions of ischemia and biliarydilatation

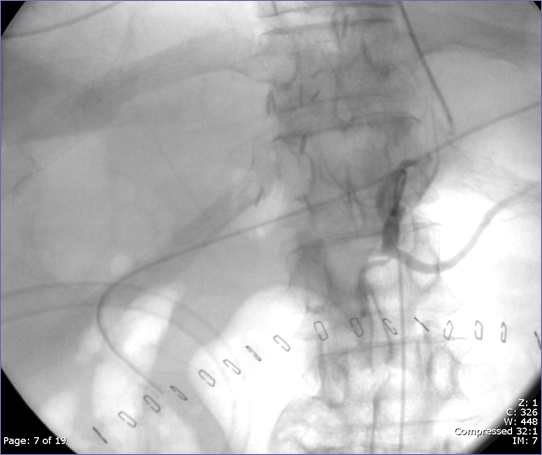
CTA: Hepatic artery stenosis
Catheter angiogram
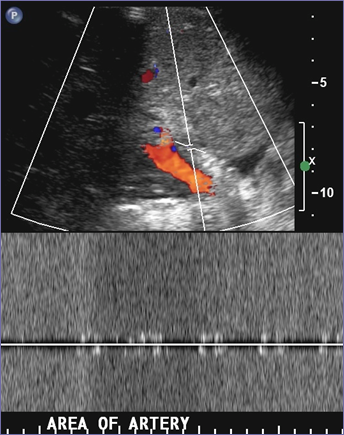
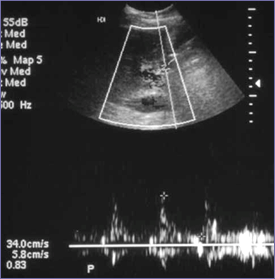
Splenic artery steal, HASwith slow HA inflow

Early
Late
Mid
Post hepatic artery angioplasty andsplenic artery embolization: normalization of resistive index, higher velocitiesgradually decreasing size of spleen
9-24
12-23
Splenic Artery Steal Syndrome
•Shunting of hepatic artery flow to splenic artery
•Clinically significant shunting may be due to factors thatincrease hepatic artery resistance (prolonged ischemictime and acute rejection)
•Portal hyperperfusion from pre-existing hypersplenismmay contribute
•Doppler will show increased hepatic artery resistiveindex and high portal vein velocities
•Splenic artery > 4mm or 150% of hepatic artery issuggestive.
•Tx: usually transcatheter splenic artery embolization
Sanyal, Shah. JUM 2009;28:471
Hepatic Artery waveformsImmediate 6 months
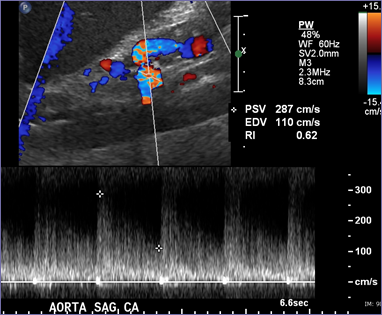
Median Arcuate Ligament Syndrome

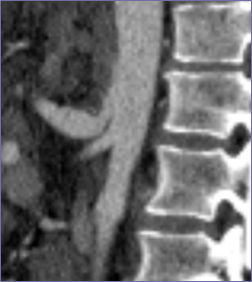
Celiac Artery Stenosis
•Causes: atherosclerosis, median arcuate ligament
–Median arcuate ligament formed by fibers of left and right cruraand can compress celiac axis
•Often asymptomatic before transplant because of richcollateral blood supply
•After tx, flow increases in celiac because of new liverand severed collaterals and patient may becomesymptomatic
•Unclear if median arcuate ligament significantlypredisposes to HAT after transplant and whether itshould be ligated at time of transplantation
Jurin, etal. Ann Surg 1993;18:10
Dravid, etal. AJR 1994;163:585
Hepatic Artery Pseudoaneurysm
Septicemia post transplant

Intrahepatic PSA treated with thrombin
Same patient several days later
Hepatic Artery Pseudoaneurysm
•Uncommon complication 0.3 – 1.2%
•Usually at anastomosis, usually mycotic, intrahepaticPSA 2 biopsy
•Imaging: use color and pulsed Doppler for a new cysticmasses, lesions will enhance on CT and MR
•May rupture spontaneously, treatment includes:
–Surgical resection and vascular reconstruction
–Embolization
–Endovascular stent
Caiado, etal. Radiographics 2007;27:1401
Strange, etal Transplant Proc 2000;32;533
Portal Vein Complications
•Thrombosis and stenosis occur in 1 – 2% oftransplants
•Causes include: faulty surgical technique,misalignment or excessive vessel length,hypercoagulable states, previous portal vein surgery,large residual varices with steal effect
• any variation in standard anastomosis
•Clinical: portal hypertension, hepatic failure, edema,massive ascites
•Treatment: angioplasty, thrombolysis, stent, surgicalcorrection with thrombectomy or jump graft
Mullan, etal. AJR 2010;195:1438
Settmacher, etal. Clin Gtransplant 2000;14:235
Wozney, etal. AJR 1986;147:657
Peri-operative PVT with flow re-established after thrombectomy
US and CT 4 days post tx
One day post thrombectomy
Intra-op after thrombectomy
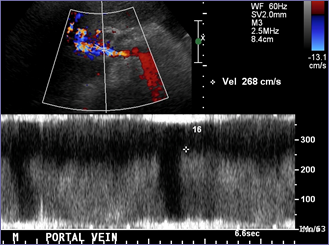
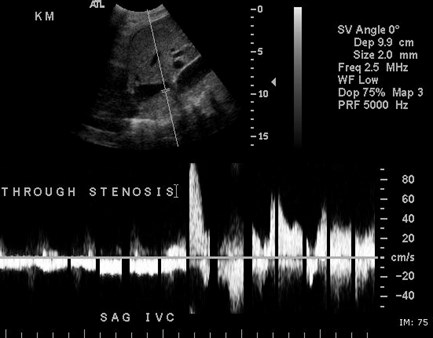
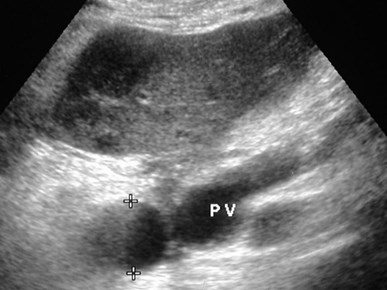
Portal Vein Stenosis
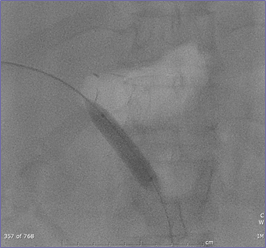
PRE
POST
Portal Vein Angioplasty


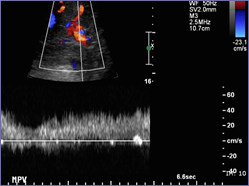
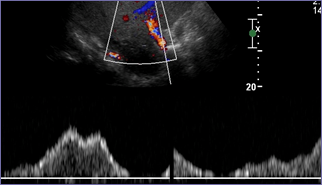
Portal Vein Stenosis
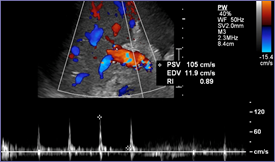
•Peak systolic velocity > 80 - 150 cm/sec OR
•Anastomotic to pre-anastomotic velocity ratio of 3:1 or4:1, have specificity of 95% or greater for PV stenosis
•Signs of portal hypertension are supportive evidence:splenomegaly, varices (may result in lower PVvelocities), ascites
•Narrowing of portal vein to < 2.5 mm
•Treatment: balloon angioplasty and/or stent placement
•A difficult diagnosis with further evaluation and treatmentdepending upon clinical findings
Mullan, etal. AJR 2010;195:1438
Vaidya, etal. US Quarterly 2007;23:239
Shibata, etal. Radiology 2005;235:1078
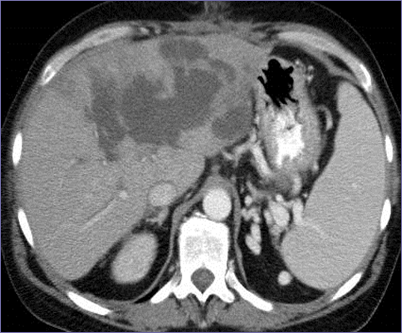
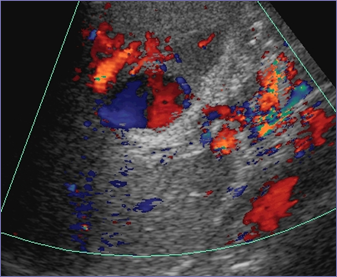
5 months post transplant-Portal Vein Thrombosis
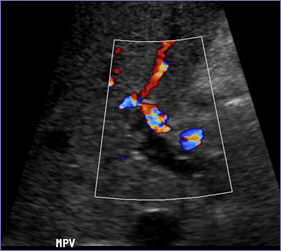
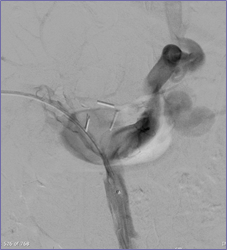

Acute thrombus
large coronary varices
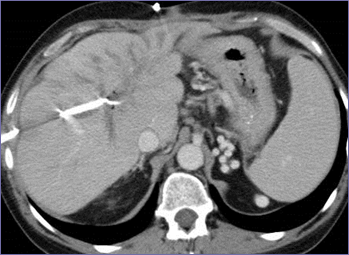
Embolization of varices and angioplastyof portal vein re-establishes flow
Poor portal vein flow in perioperative periodPatient returned to OR
Day 1
Day 2
Despite revising anastomosis,intraoperative flow is very poor
Large splenorenal varices shunted flow from PVLigation of varix improved PV flow

Pre-operative imaging
Horrow, etal. JUM 2010;29:125
Suggestions and Tips
•Pre-operative CTA: PVT, anatomic variations, celiac stenosis,size of splenic artery, size of varices (spleno-renal
•Talk to surgeons
–Unusual anastomoses and donor anatomy
•Do not have tunnel vision and only do liver images withDoppler. Measure spleen, look for varices, celiac stenosis
•Combinations of complications may occur
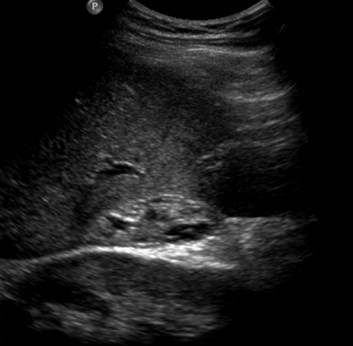
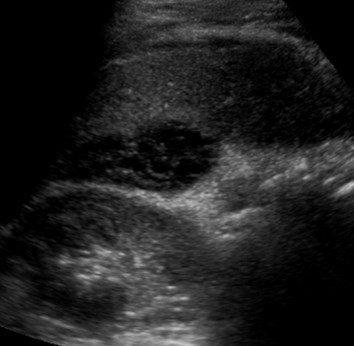
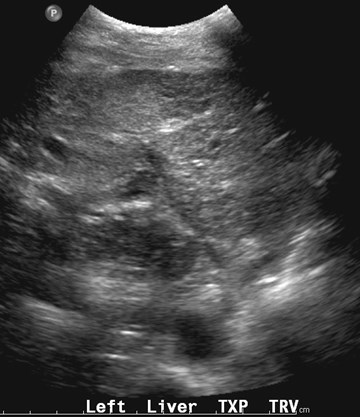
•Use gray scale images, especially for signs of ischemicliver parenchyma or bile ducts
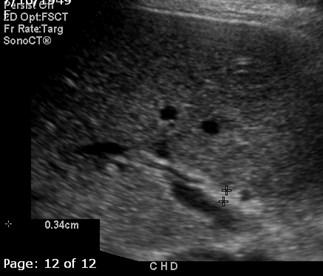
–Sludge in bile ducts may be isoechoic or just slightly moreechogenic than liver, may see isolated areas of biliary dilatation
•If high index of suspicion for vascular complication andUS negative, get CTA, MRA or catheter angiography
IVC Complications
•Thrombosis and stenosis relatively rarecomplications in < 1%, more common in childrenand after re-transplantation
•Stenosis- 3-4 times increase in velocity
•Other US findings in stenosis include ascites, pleuraleffusions, hepatomegaly
•Significant supra hepatic caval stenosis may resultin reversed flow or loss of phasicity in hepatic veins
•Thrombus may be partial or occlusive, hypo orhyperechoic
Mild IVC anastomotic stenosis


Recent transplant

Left hepatic vein and partial IVC thrombus

Several months later
Thrombus Resolved
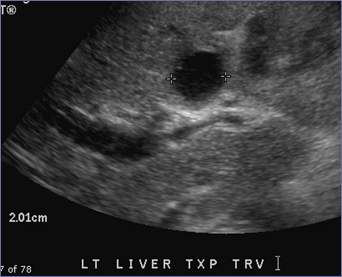
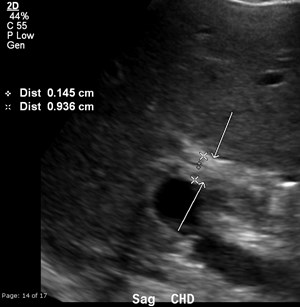
Biliary Complications
Abnormal LFTs several months aftertransplant
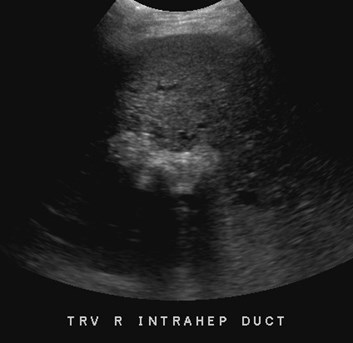
Right lobe

Left lobe

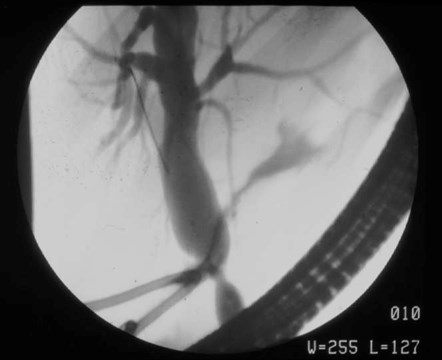
Anastomotic Stricture


Initial ERCP
Post biliary dilatation


Abnormal LFTs

Stricture at bile duct anastomosis with biloma
Biliary stricture develops over timesecondary to arterial ischemia

5-2
6-9
7-8
Hepatic artery thrombosis
Arterial collaterals
Celiac angiogram
6 months later
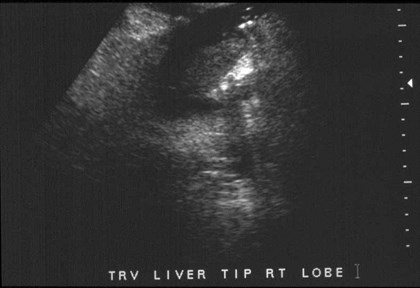
Gray scale images of liver

Post HAT biliary strictures and sludge
Abnormal LFTs


Liver Biopsy: acute cellular rejection andpericholangitis with ductal intraepithelial infiltrateconsisting of lymphocytes, plasma cells andneutrophils



Partially calcified biliary sludge

Several months after documented HAT
Biliary Complications
•Incidence: 10-33%
•Most occur within 6 months of tx
•Obstruction, leak, sludge and stones
•Strictures
–Anastomotic- secondary to scar tissue
–Non-anastomotic- often ischemic 2º hepatic a. abnormality
–(Blood supply to proximal duct and intrahepatic ductsderives solely from reconstructed artery
•Imaging
–US sensitivity for dilatation reported as 50 – 60%(likely because sludge filled ducts and stricturesare difficult to appreciate)
–Cholangiography (ERCP, MRCP) is definitivestudy
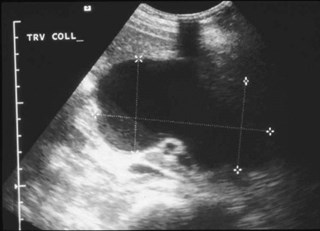
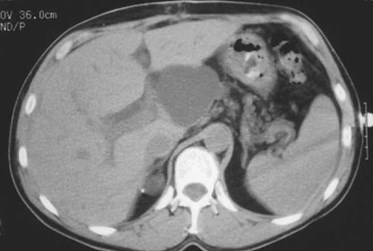
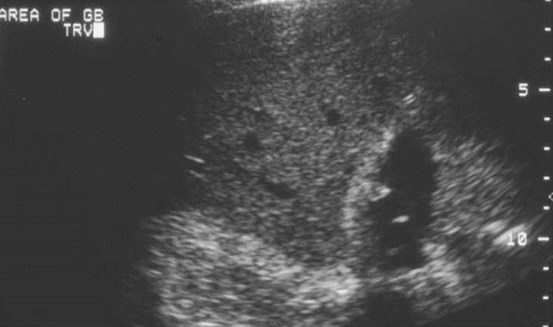
Miscellaneous Complications
Acute hematomadifficult to appreciate because isoechoic with liver
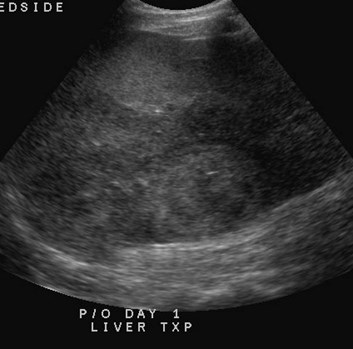
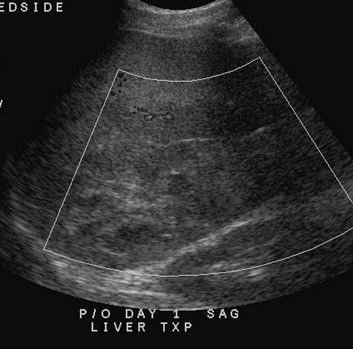
Immediate post operative imaging
Intra and extra-hepatic hematomas

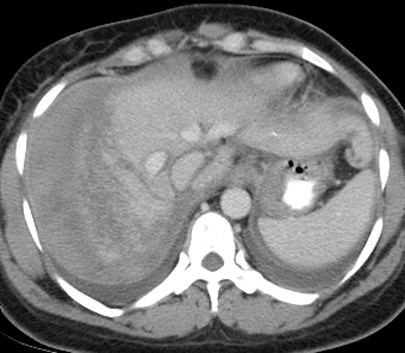
Immediate post operative imaging

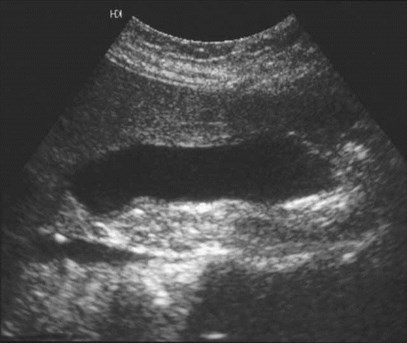
Mucocele of cystic duct remnant
Mucocele of Cystic Duct Remnant
•Very rare complication
•Occurs when donor cystic duct with loworigin is incorporated into the surgicalanastomosis
•Mucus produced by remnant has noegress, accumulates under tensioneventually compressing adjacent bile duct
Abcarian, etal J. Vasc Interven Radiol 5:127-130, 1994
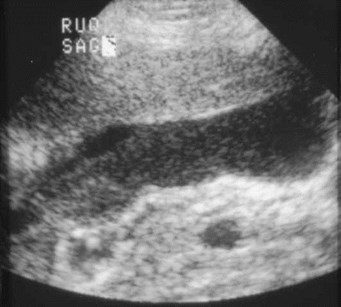
Small subhepatichematoma, 3 days aftersurgery
Repeat study 1 weeklater with fever
PerihepaticAbscess

Perihepaticabscess


US and CT several daysafter transplantation
1 week later without therapy
Surgicel simulates an abscess


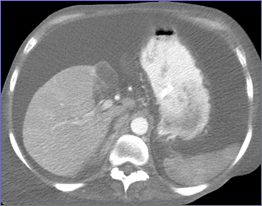
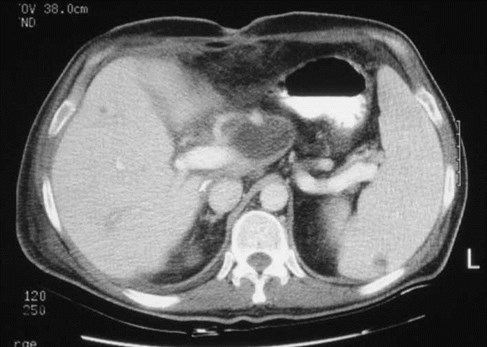
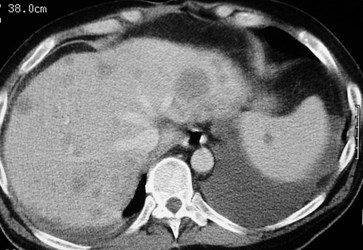
Infarcts with necrosis
Infarcts
•Variable appearance. May be round orgeographic, usuallly hypoechoic orhypodense, but solid. May contain gas,even without infection.
•Appearance may overlap with abscess,which tends to have thicker walls, but mayalso be hypoechoic and contain gas.


Abdominal painone week posttransplant
AcutePancreatitis

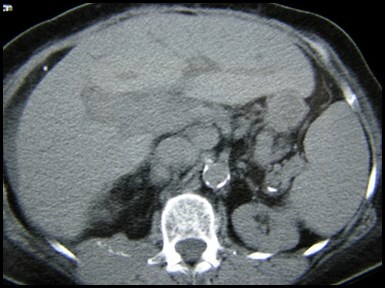
6 months after transplant with abdominal pain and fever
Liver sag trv
spleen
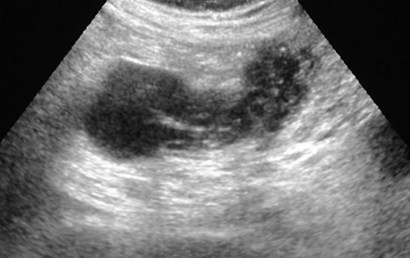

Lymphadenopathy,thickened small bowel
jejunum
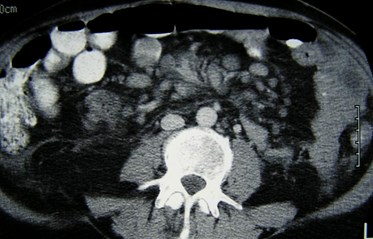

Post TransplantationLymphoproliferative Disorder
•Interaction of Epstein-Barr virus with weakimmune system
•Results in spectrum of disease from benignpolyclonal lymphadenopathy to malignantlymphomas
•Occurs in 2.2% of liver transplant patients
•Lymphomas in cyclosporine treated patientsoccur 4-6 months post transplant withwidespread involvement at presentation
PTLD
•Nodal and extra-nodal involvementespecially tonsils, GI tract, liver, thorax
•Enteric lesions have increased incidenceof ulceration and perforation
•If detected early and treated with reductionin immunosuppressive agents, most casesresolve
Wu, etal. Abdom Imaging.2001;26:200-206
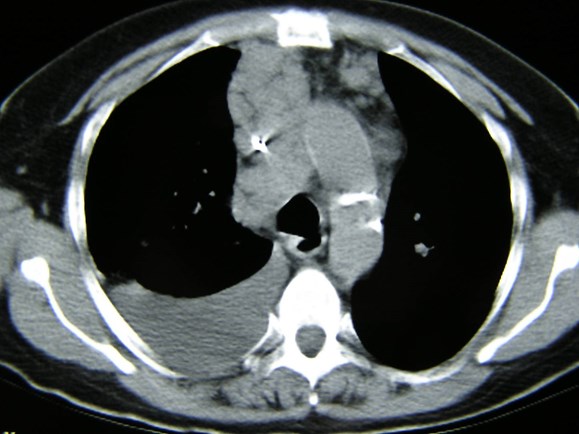
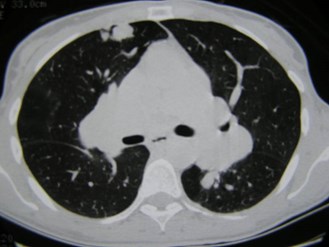
Chest CT for unexplained pleural effusion, explanted liverhad hepatocellular carcinoma

Recurrent hepatocellular carcinoma in liverwith metastases to mediastinum, pleura,bone, lymph nodes, adrenal gland
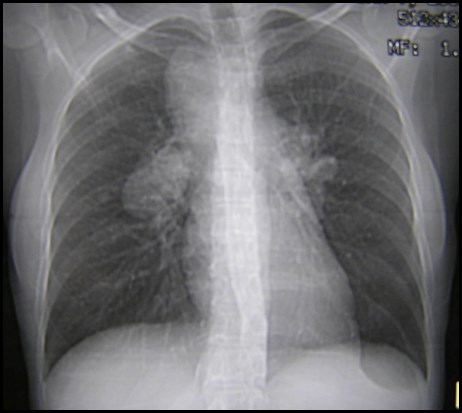
Original transplant for HCC, now with abnormal CXR

Recurrent Hepatocellular CA
•Lungs most common site of recurrence, 2nd mostcommon liver allograft. Then abdominal lymphnodes and bone.
•Rare to see recurrence in Stage 1 or 2 disease
•Recurrence 4x more common with Stage 4 than3
•CT more sensitive than tumor markers
Ferris, etal. Radiology 1996;198:233-238
Katyal, etal. Radiology 2000;216:698-703
Other Issues
•Rejection: US appearance is non-specific. Only findingmay be parenchymal heterogeneity. Waveforms do notnecessarily correlate.
•Re-infection with hepatitis C virus: occurs in nearly alltransplants. Benign in short and medium term in mostpatients (80-85%)
•Small subset will develop fibrosing cholestatic hepatitis,progressing rapidly to liver failure.
•Autoimmune hepatitis may recur. These patients needhigher levels of immuno suppresion to preventrecurrence.
Keefe EB. Clin Liver Dis 2000;4:241-255
The End
